Defending Claims Involving Future Radiofrequency Neurotomy TreatmentsTIDA Newsletter - Fall 2018
By John Crawford and Lauren Nuffort Plaintiffs in personal injury actions often claim they will need future radiofrequency neurotomy (RFN) treatments indefinitely to obtain relief from chronic neck or back pain and to improve function and quality of life. These claims create the potential for significant future damage awards. However, data from a plaintiff’s own doctor often does not support such a claim. Instead, the data reveals that patients often discontinue RFN treatments after the third or fourth procedure. The defense should seek to obtain that data during discovery to discredit testimony by a plaintiff’s pain specialist and support a motion in limine to preclude such testimony altogether. What is a Radiofrequency Neurotomy? A radiofrequency neurotomy is an injection most commonly given to individuals with facet joint pain, such as low back pain, neck pain, and thoracic and sacroiliac joint pain. Tyler J. Christensen et al., Outcomes and Prognostic Variables of Radiofrequency Zygapophyseal Joint Neurotomy in Utah Workers’ Compensation Patients, 10 J. Pain Research 1207, 1208 (2017). The terms radiofrequency ablation and radiofrequency rhizotomy are used interchangeably with radiofrequency neurotomy. The outpatient procedure involves the application of heat generated by radio waves to target specific peripheral nerves, cauterize them, and temporarily interrupt the nerve’s ability to send pain signals. Radiofrequency Neurotomy, Mayo Clinic, https://www.mayoclinic.org; See also Wheatley v. Cohen, No. 14 C 5161, 2016 WL 183915, at *2, fn. 2 (N.D. Ill. Jan. 13, 2016). A peripheral nerve, however, regenerates. As such, the pain someone experiences can return when the nerve regrows. Eun Ji Choi, et al., Neural Ablation and Regeneration in Pain Practice, 29 Korean J. Pain 3 (2016). For this reason, both plaintiff and defense medical experts may opine that the benefits experienced from an RFN wears off when the nerve regenerates, and future RFNs may be needed for the plaintiff to have ongoing relief from chronic pain. Typical Claims by Plaintiffs Regarding Future Treatments: When a plaintiff finds that conservative remedies do not provide the intended pain relief, the treating doctor may recommend a radiofrequency neurotomy. As a baseline argument, plaintiffs’ treating pain management doctors point to the generally accepted fact in the medical community that cauterized peripheral nerves regenerate after a period of time. Brian Rambaransingh et al., The Effect of Repeated Zygapophysial Joint Radiofrequency Neurotomy on Pain, Disability, and Improvement Duration, 11 Pain Med. 1343, 1343–1347 (2010). Pain management doctors therefore generally agree that an RFN is not a permanent solution and pain recurrence can happen when the treated nerves regenerate. Id. If the pain recurs, the patient can repeat the treatment to reinstate the relief. Treating pain management doctors rely on clinical studies that have shown that repeating RFN treatments has been successful in 85 percent of patients who had a successful initial injection. Id. In these studies, success was defined by greater than or less than 50 percent pain relief and by the patient’s desire to have the RFN repeated. Id. On average, successful RFN treatments relieved pain for eight to 13 months before the nerve regenerated. Jerome Schofferman et al., Chronic Whiplash and Whiplash-Associated Disorders: An Evidence-Based Approach, 15 J. Am. Academy of Orthopaedic Surgeons, 596, 596–606 (2007); Paul Dreyfuss et al., Efficacy and Validity of Radiofrequency Neurotomy for Chronic Lumbar Zygapophysial Joint Pain, 25 Spine 1270, 1270–1277 (2000); Greg McDonald et al., Long-term Follow-Up of Patients Treated with Cervical Radiofrequency Neurotomy for Chronic Neck Pain, 45 Neurosurgery 61, 61–68 (1999). Plaintiffs’ pain management doctors consistently testify in favor of repeating RFNs. In a 2017 decision issued by the Texas Court of Appeals, Oney v. Crist, 517 S.W.3d 882, the plaintiff’s doctor testified to the following:
In a personal injury case filed in the U.S. District Court for the Middle District of Louisiana, the plaintiff’s economist opined that it would cost more than $350,000 for the plaintiff to have the procedure repeated for the remainder of his life, even though the plaintiff’s pain management doctor never testified that the plaintiff would experience relief for the rest of his life by repeating them. Important Evidence that the Defense Should Obtain During Discovery: Subpoenas to pain specialists and their clinics requesting data on the number of repeat RFNs can reveal data which undercuts a plaintiff’s claim he or she will need future RFNs indefinitely. Consider including the following topics with your subpoena to a pain management clinic:
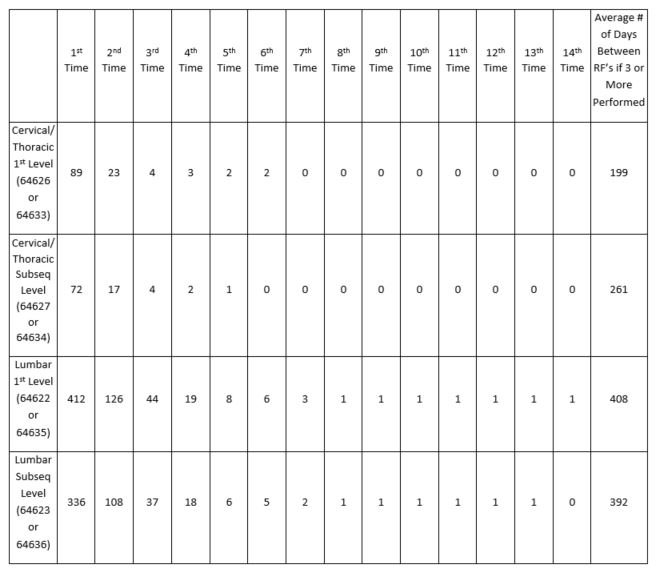
By referencing specific current procedural terminology codes, a subpoena forces the pain specialists and their offices to produce the relevant data, and it prevents them from objecting to the subpoena on the grounds that the request is too onerous. The data generated in response to these subpoenas can reveal that the plaintiff is unlikely to have RFNs indefinitely. For example, the authors of this article served subpoenas on two pain management clinics requesting the data discussed above. In that case, the plaintiff’s pain specialist opined that the plaintiff would need to repeat RFN treatments once a year for the rest of the plaintiff’s life. Specifically, that doctor stated in his narrative report the following: [Plainitff’s] chronic neck pain has been present for over four years and has not resolved with time or conservative therapy. Therefore, to a reasonable degree of medical certainty his neck pain will not spontaneously resolve. That neck pain is, in fact, permanent and will require repeat radiofrequency ablation procedures on approximately an annual basis for the remainder of his life if he wishes to have relief for that chronic pain. In response to a subpoena, the clinic where the plaintiff’s pain specialist practiced, referred to here as XYZ Anesthesiology, produced a summary of the RFN treatments that the clinic performed between 2006 and 2015. The summary showed that 89 individuals had an RFN at one cervical or thoracic level. Of those, 23 patients had a second, four had a third, and none had more than six total. The average number of days between the treatments for patients who received three or more was 199 days. See Table 1, below. Table 1. XYZ Anesthesiology Level of RF Not Taken Into Consideration
Motions in Limine to Exclude Testimony About Future Treatments: Defendants facing claims of future damages for radiofrequency neurotomy treatments should move to exclude the testimony of a plaintiff’s doctor on the grounds that it does not meet the standard of admissibility. See, e.g., Fed. R. Civ. P. 702. In federal cases, the trial court must determine whether the expert’s testimony “rests on a reliable foundation.” Daubert v. Merrell Dow Pharm., Inc., 509 U.S. 579, 597 (1993). In cases involving claims for future RFNs, the defense should argue that while a doctor’s report indicates that the plaintiff will need annual treatments for the rest of his or her life, that opinion is not supported by any medical literature that shows that patients receive treatments for that period of time and it is inconsistent with the statistics from the doctor’s own clinic. The expert’s claims are therefore speculative and counter to the available evidence, and the court should prohibit the doctor from testifying that the plaintiff will need future, indefinite RFN treatments. Conclusion: Defense attorneys should follow a systematic approach to defend against plaintiffs’ claims for indefinite, future RFNs. It is important for defense attorneys to recognize at the outset of their cases that their IME doctors will probably agree that RFNs may only provide temporary relief from pain caused by a facet injury and that it may be reasonable to repeat it when the pain returns. The IME doctors may also concede that clinical studies have shown that patients who have undergone successful RFNs will likely experience the same success on repeating them. Therefore, to dispute plaintiffs’ claims for unlimited future RFNs, it is important for defense counsel to subpoena data from the plaintiff’s pain specialist to show that almost all of his or her own patients cease getting them after three or four procedures. Such data may very well preclude the plaintiff’s pain specialist from testifying that the plaintiff will need future RFNs.
About the writers:John Crawford, who has been a TIDA member since 1998, practices law in Minnesota and Wisconsin. His litigation experience in commercial trucking includes claims for wrongful death, personal injuries, traumatic brain injuries, punitive damages, cargo liability, broker liability, loading/unloading accidents, and premise liability. He also assists clients with pre-suit investigations, including document collection and preservation. He is certified as a civil trial specialist by both the National Board of Trial Advocacy and Minnesota State Bar Association. Since 1997, he has served as the editor of the 26-chapter Minnesota Insurance Law Deskbook. Lauren Nuffort’s practice areas include transportation litigation, construction litigation, professional liability defense, property and catastrophic loss, as well as a national property subrogation practice. She is co-founder and current co-chair of the Minnesota Defense Lawyers Association Women in the Law Committee.
Return to Newsletter |


TIDA Partners






Upcoming Events
Tue Jun 23, 2026TIDA Webinar: A Tale of Two Cities: Subrogation Plaintiff and Defense Lawyer Insights on Subrogation Claims Category: Webinars |